What are one-way valves?
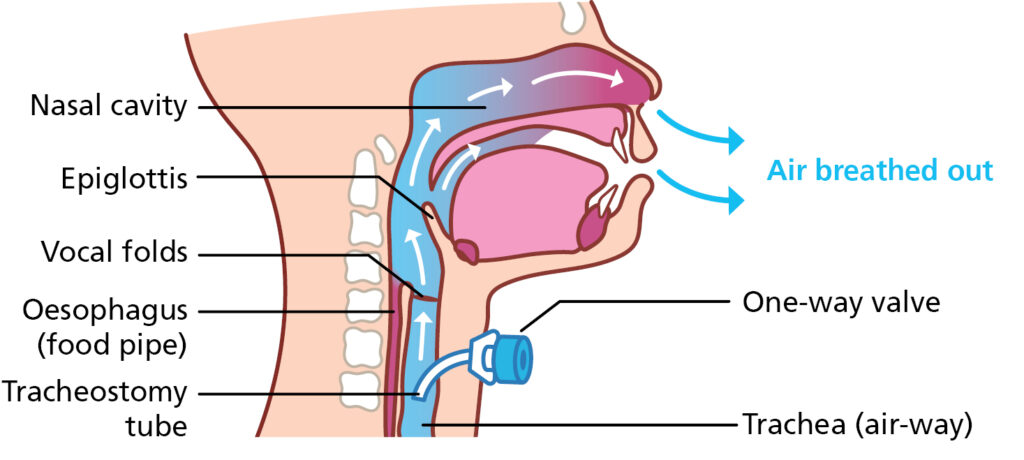
A one-way valve is a plastic attachment that fits on the end of your child’s tracheostomy tube. This allows your child to breathe in through their tracheostomy tube and when they breathe out the airflow is diverted back up through the upper airway.
Not all children will be able to tolerate a trial or wearing a one-way valve, it depends on their airway difficulties, you can ask your child’s doctor or nurse about this.
breathing in

breathing out
Potential benefits of a one-way valve
There are lots of benefits to having a one-way valve.
Communication
- Voicing – helps development of early language skills in babies and young children
- Louder / clearer voice in older children
- The ability to say more words on one breath
Swallowing
- Improved sense of taste and smell
- Make the swallow more effective
Other benefits
- Helps the child become aware of their own secretions which they can then clear with a cough and a swallow
- Helps the child get used to normal airflow again which helps in the process of removing the tracheostomy when appropriate
- Bearing down – e.g. lifting, bracing, toileting
Disadvantages of wearing a one-way valve
There are very few disadvantages but you or your child may notice the following:
- Increase in the effort needed to breathe out
- It may take your child a while to get used to it, they may therefore need to gradually build up the amount of time wearing the valve
- Some children produce thicker secretions as the valve does not humidify the air when your child breathes in. You may need to alternate use of the speaking valve with an HME/Swedish nose. Some children also need to use nebulisers
What happens at the appointment?
There will be a Speech and Language Therapist and a Specialist Nurse at the appointment. They will make your child feel comfortable and distract them by doing an activity to suit their age.
The valve trial
You will be asked to suction your child’s tracheostomy tube so that their airway is nice and clear to optimise airflow. You will be asked if your child makes any sound already, this is to check whether they have any leaked airflow around their tracheostomy tube.
We will then ask you to remove the Swedish Nose from the end of the tracheostomy and we will place a gloved finger on the end of the tracheostomy to see how well this is tolerated by your child. We might use a mirror too to see if there is any leak around the tracheostomy, we will see the mirror “misting” if that is the case. Following this we will then place the valve on the end of the tracheostomy. It may take a few attempts for your child to tolerate the valve. We will observe your child to see if it is safe to take the valve home with you.
There will be plenty of time for you to ask questions and find out how to use and care for the valve should your child be given one to take home.
If you can take the valve home we will give you written advice on how to use and care for the valve. It will also have the order code for the valve so that your child’s community nursing team can order replacement valves. Your child’s Speech and Language Therapy team will also get a copy.
Where to come
You need to bring your child to the:
ENT department, C Floor, Brotherton Wing, LGI
Please let the receptionist know when you arrive.