This leaflet provides information for parents and carers about Transposition of the Great Arteries in children and the management and treatment of this condition.
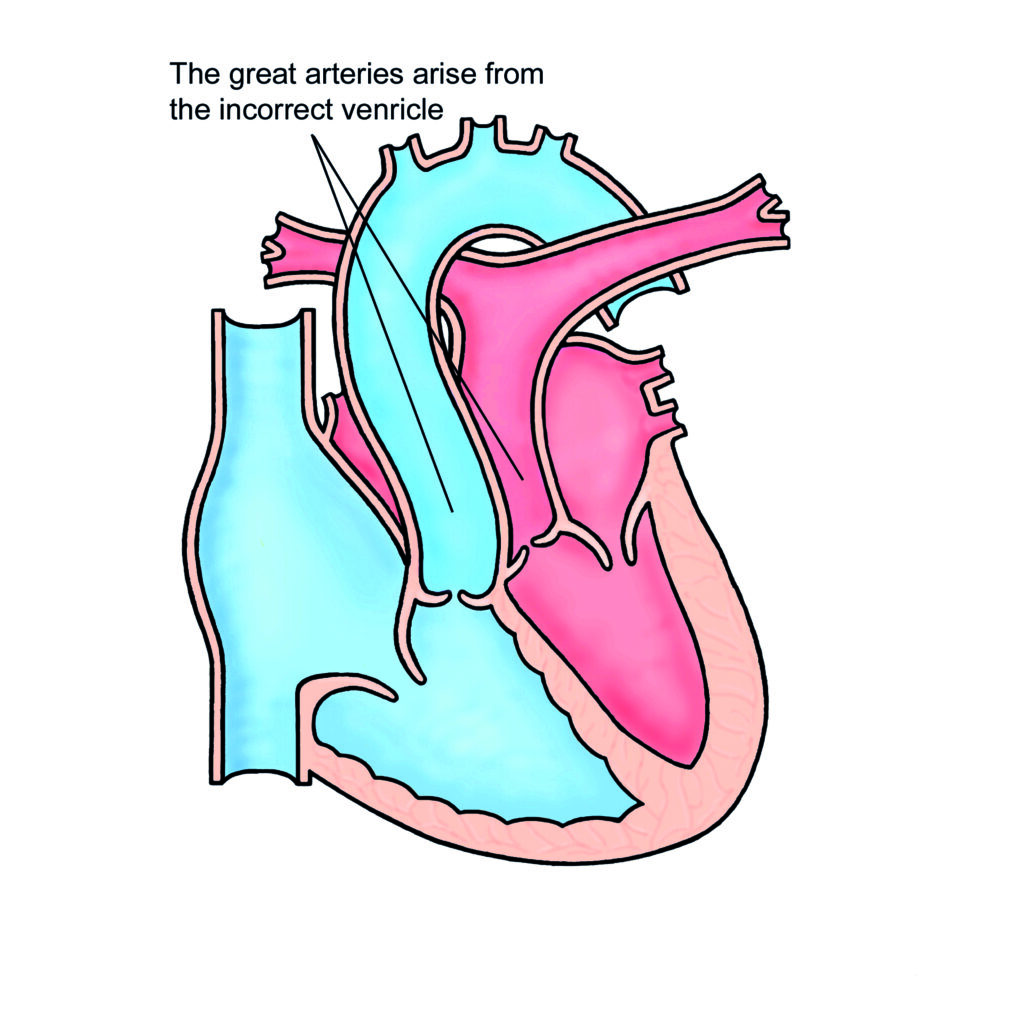
This is a serious heart condition in which the main artery which should arise from the right side of the heart comes from the left side, and the artery which should arise from the left side of the heart comes from the right side.
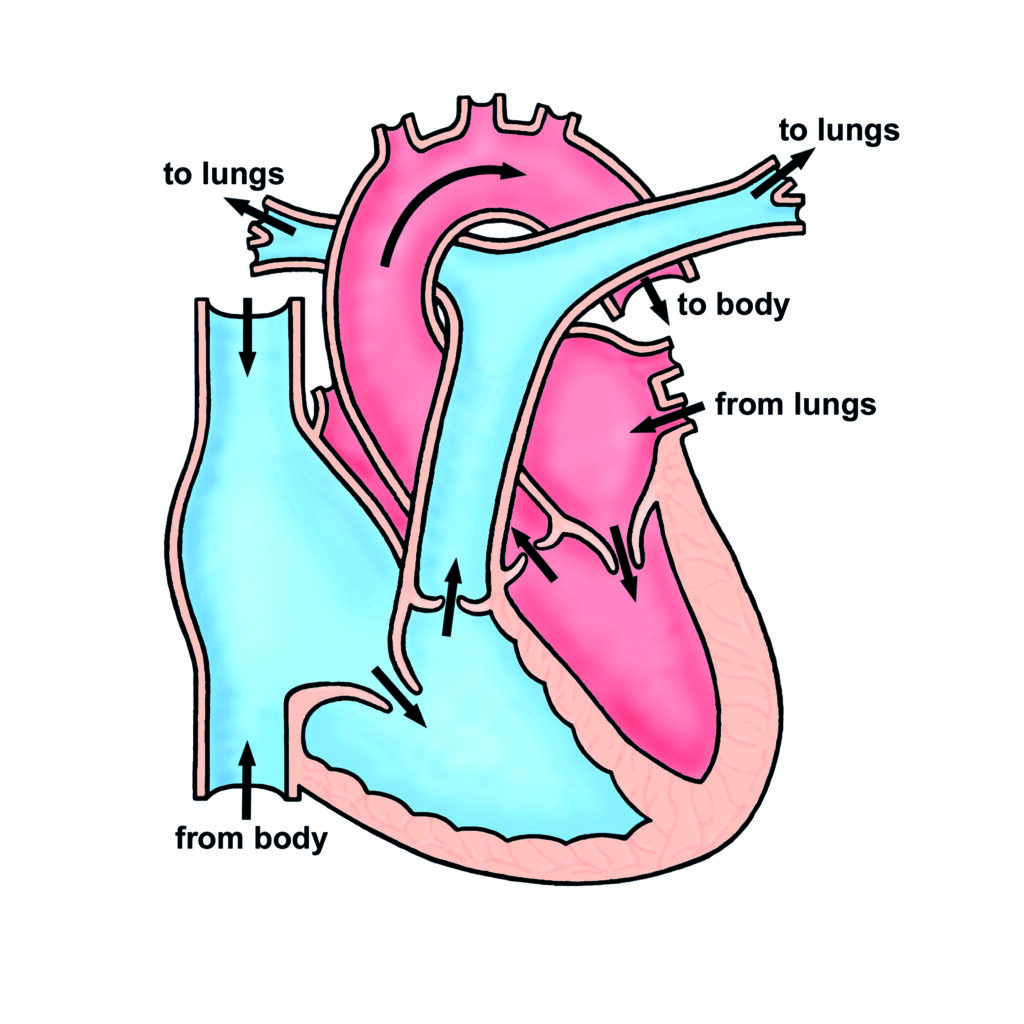
In the normal circulation blue blood, in which the oxygen has been used up by the body, drains to the right side of the heart which pumps the blood to the lungs. In the lungs oxygen is collected, making the blood pink (or “oxygenated”). The pink blood is then returned to the left side of the heart which pumps the pink blood to the body.
In a baby with Transposition of the Great Arteries the blue blood gets pumped back to the body instead of to the lungs, the baby appears blue shortly after birth and may die quickly without treatment.
Transposition of the Great Arteries – YouTube. Transcript
This video explains the condition transposition of the great arteries or
TGA for short and its treatment you may find it helpful to look at our video of the normal heart before watching this video in the normal circulation blood that is low in oxygen returns from the body in veins to the right side of the heart where it is pumped from the right ventricle to the lungs through the
pulmonary artery plant picks up oxygen in the lungs and returns to the heart where it is pumped from the left ventricle to the body through the aorta the aorta and pulmonary artery are together referred to as the great arteries shortly after the aorta leaves the heart it gives off two branches the coronary
arteries that supply the heart itself with blood in transposition of the great arteries the aorta and pulmonary artery are connected to the heart the wrong way round this means that blood returning from the body that is low in oxygen is pumped out of the right ventricle to the aorta and
so back around the body at the same time blood returning from
the lungs that has lots of oxygen is pumped from the left ventricle to the pulmonary artery and back to the lungs the consequence of transposition of the great arteries is that oxygen cannot be delivered to the body and unless treated quickly the baby is unlikely to survive the immediate priority is to ensure that at least some oxygenated blood can get to the body when a baby is born there is a natural hole called a patent for a monovale between the two collecting chambers of the heart the right atrium and the left atrium often this hole is not wide enough so a procedure called a balloon atrial septostomy is performed a tube is inserted through a vein in the groin into the right atrium and across into the left atrium once in the left atrium a balloon is inflated and pulled back into the right atrium this enlarges the hole between the right and left atria and so allows for more oxygenated blood to be pumped around the body by improving the delivery of blood to
the body this procedure buys some time until a corrective operation can be
performed although not illustrated here oxygenated blood can also pass between the aorta and pulmonary artery through a small connection between the two arteries called the ductus arteriosus the ductus arteriosus is open when a baby is in the womb but usually closes shortly after birth a baby with transposition of the arteries might be given a drug to keep the ductus arteriosus open until a balloon atrial septostomy or a correction operation are performed surgical correction of transposition of the great arteries is achieved by performing an arterial switch operation usually in the first few weeks of life after opening the chest through the middle of the breastbone the coronary arteries are detached from the aorta and both the aorta and pulmonary artery are cut just above where they leave the heart each artery is moved and reconnected to the correct side of the heart the aorta to the left ventricle and the pulmonary artery to the right ventricle the coronary arteries are then reconnected to the aorta in its new position the arterial switch operation therefore results in a normal circulation with oxygenated blood being pumped from the left ventricle to the body via the aorta and blood that is low in oxygen being pumped from the right ventricle to the lungs via the pulmonary artery lifelong follow-up is required after the arterial switch operation in most patients it is likely that no further operations or procedures will be required but in some patients complications occur that require further
treatment either in childhood or in adulthood
Tests
Usually an ultrasound scan (“echocardiogram”) is required to make the diagnosis.
Treatment
The first stage of treatment is to keep the baby alive by increasing the amount of oxygenated blood which gets to the body. Medicines can help to some extent and most babies will be given a drug called dinoprostone, as an injection into one of the veins. Almost all babies with Transposition of the Great Arteries will also need a procedure called a “balloon septostomy” to make sure they get enough oxygen to their body to survive. This involves putting a tube with a small balloon at its tip into the vein at the top of the leg or in the umbilicus. The tube is passed up into the heart and across the flap of heart tissue which separates the two small filling chambers, using an ultrasound scan to see it is in the correct position. The balloon is then inflated and the catheter is pulled back across the flap, tearing a hole in it and allowing oxygenated blood to cross from the left side of the heart to the right side.
Once the baby is safe, we can plan the baby’s operation to “switch” the arteries. The switch is usually done within the first two weeks after birth. Most babies are well enough to go home 5-7 days after the operation. Prior to surgery, the surgeon will discuss the operation in more detail including the risk and potential complications.
Complications can sometimes occur late, even many years after a successful switch operation, and it is important to have occasional but regular visits to the outpatient clinic to make sure all is well as the baby grows and even throughout adult life too.
Late problems which can arise include narrowing of the arteries leading to the lungs (the pulmonary arteries), leaking heart valves (most commonly the aortic valve), and narrowing of the small arteries (the coronary arteries) which feed blood to the heart muscle. These complications are all rare but can be serious enough to need further surgery or keyhole treatment.
General advice for the future
Most children lead a normal active life after a switch operation, including sports. If there are any particularly strenuous activities to be avoided your cardiologist will let you know.
All patients who have had a switch operation will be at risk of infection in the heart (called endocarditis) after surgery. Such infections may be caused by infections of the teeth or gums. It is important to visit the dentist regularly (every 6-12 months). Ear or body piercing and tattooing are best avoided as they also carry a small risk of infection which may spread to the heart.
For more information about endocarditis please see the link below: