The human ear has three parts:
- The Outer Ear
- The Middle Ear
- The Inner Ear
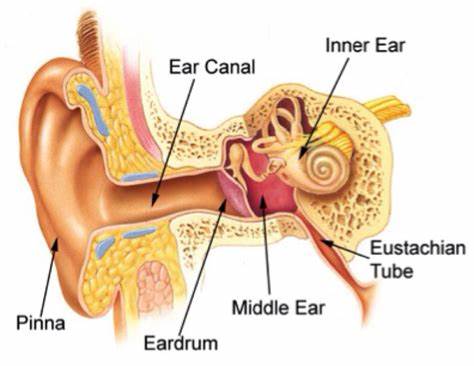
The Outer Ear consists of the Pinna, the external auditory meatus (or ear canal) and the tympanic membrane or ear drum.
The outer ear is mainly made up of bone and cartilage. The outer 2 thirds of the ear canal is covered with tiny thin hairs and the inner third of the canal to the ear drum is smooth skin with glands that secrete cerumen or as better known; Ear Wax.
This smooth skin is naturally migratory, which means that it moves on its own. When this happens, the wax that has been secreted by the glands of the smooth skin collect any dust or debris from the ear canal which could be harmful to the ear drum. Eventually this movement will mean that the wax falls out of the ear.
To learn more about ear wax and how you can maintain it, please see our page on ‘Ear Wax’.
The Tympanic Membrane or Ear Drum is a thin piece of skin at the end of the external auditory canal which moves to changes in pressure externally. The outer ear and the ear drum are the first part of our hearing pathway, or the initial conduction of sound.
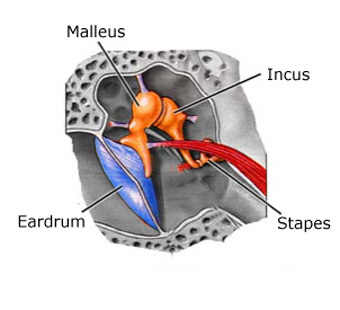
The second part to the ear is the Middle ear, housed behind the ear drum. This is a cavity that is linked with our nose via the Eustacian tube, and helps to maintain the correct pressure in our ears.
Inside the cavity are three tiny bones that are linked together. These bones are the smallest bones in our body and are called the Ossicles. These are the Malleus, Incus and Stapes, (or Hammer, Anvil and Stirrup). These tiny bones begin to move along with the eardrum when there has been an external pressure change (sound source). This is our second part of our hearing pathway, and the second part to the conduction of sound.
The Inner Ear is where our organ of hearing is found; the Cochlea.
The Cochlea is a snail shell shaped organ which is found within the skull, or the mastoid bone of the head. It is a tiny organ around 9mm in diameter (or around the size of your little fingernail).
The Cochlea houses thousands of hair cells that transmit signals to the Brain when stimulated.
When the ear drum and ossicles vibrate, the footplate of the Stapes pumps into the Cochlea via a small hole called the Oval window. This action sets off a motion inside the Cochlea like a wave stimulating the membrane the hairs sit in. Any hairs that are stimulated by this motion send a signal to the Brain through a nerve called the Vestibulocochlear Nerve. The Brain then interprets the signal and we then ‘hear’ the sound that made the pressure change. This is then our neurological (nerve) hearing pathway.
What do I do if I think my hearing has changed?
If you have experienced a sudden change in your hearing, such as waking up with a deafness, a drop in hearing in one ear over a short period of time, or a deafness with pain or discomfort including discharge from the ear, we would suggest seeking medical advice immediately. This would be from your GP or from the Accident and Emergency department at your local hospital.
There are three types of hearing loss that you could experience.
- Sensorineural Hearing Loss
- Conductive Hearing Loss
- Mixed Hearing Loss
There are also grades of hearing loss:
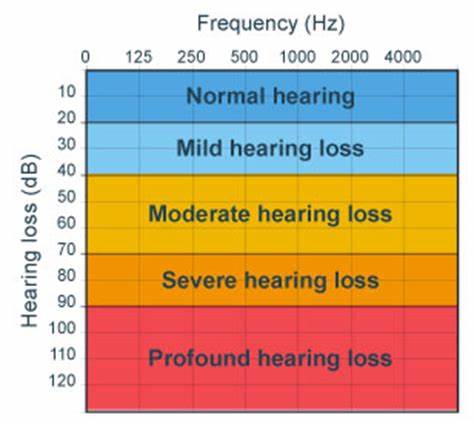
Hearing assessment is carried out in a quiet or soundproof environment. The test is to determine the quietest sound you are able to hear using either a pure tone or a warble tone. Your audiologist will explain the test to you on your arrival and discuss your results with you. The further down on the graph your results are, the more severe your hearing loss is.
Sensorineural Hearing Loss
It is likely that most of us as we get older will experience a deterioration of hearing. This usually happens gradually over time. There are generally typical signs of this such as:
- Television volume up and down
- Unable to hear clearly on the telephone
- Mishearing in general conversation
- Struggling to hear in background noise
- Difficulties hearing in groups
- Hearing people talking but not understanding what they are saying
- Things are sounding ‘muffled’
This kind of hearing loss is known as Presbyacusis, or age related hearing loss. This loss affects the production of nerve signals from the organ of hearing or the Cochlea. A sensorineural hearing loss.
Overtime our ears are bombarded with sound and some of the hair cells in the Cochlea that are responsible for high pitched or ‘clarity’ sounds are damaged. This leads to a hearing loss within the high frequency sounds making things harder to understand even though we can still ‘hear’ the noise.
There can be other reasons for this type of reduction in hearing, such as:
- Noise exposure – occupational and/or leisure
- Head trauma
- Chemo or radio therapies and/or ototoxic drugs (your consultant should discuss this with you and will request a hearing test if they feel it is necessary)
- Certain medications (do NOT stop taking important medications unless you have been directed to do so from your prescribing clinician or GP)
- Acoustic Neuroma – this is uncommon and usually only affects one ear. Your consultant or audiologist will discuss this with you and a full investigation will be carried out where necessary.
If you feel that you are noticing a change with your hearing, it is always a good idea to have your hearing checked. Your GP can make a referral to Audiology or the Ear, Nose and Throat department and we will be able to inform you if you have any deterioration of hearing and what options are available to you.
Conductive Hearing Loss
Our ability to hear initially relies on how our ears manage to conduct sound to the organ of hearing (or Cochlea). Conduction of hearing starts with our outer and middle ear. If there is any damage or obstruction in these areas, our hearing will be affected.
Here are some reasons for conductive hearing loss:
- Ear infection
- Blockage of ear wax
- Perforated ear drum
- Foreign body in the ear canal (such as a bead or cotton bud)
- Dislocation of the ossicles (a break of the Middle ear bones)
- Eustachian Tube dysfunction (build up of fluid behind the ear drum) or Glue ear
- Grommet or T-Tube insertion
- Cholesteatoma (a collection of skin and cells inside the ear, usually affecting the eardrum) – this is a rare but will require attention as soon as possible.
There are different treatments depending on the type of conductive hearing loss you are experiencing. Some of the options may be:
- Hearing Aid/s – this could be a standard or implantable device option
- Medication
- Operation – this will be discussed with you if it is a feasible option
- Watch and wait – your consultant will discuss with you if this is an option
Mixed Hearing Loss
This is just a mixture of Conductive and Sensorineural hearing losses. Sometimes people will have a natural deterioration of hearing along with a small perforation for example.
Your consultant or audiologist will discuss this with you and go over all of the viable options with you.
How do I get my hearing assessed?
Other than sudden hearing loss, please see your GP in the first instance. If it is required, your GP can then send a referral to the Ear, Nose and Throat department or Audiology services. A full assessment will be carried out and all the options available discussed with you.
If you are a current Leeds Teaching Hospitals NHS Trust hearing aid user and would like your hearing and hearing aid reassessed, please arrange an appointment at one of our hearing aid repair centres where the audiologist can perform preliminary checks to ensure an assessment can proceed.
0113 5181823 – our hearing aid aftercare service booking line.
Please note
We are unable to offer hearing tests at our hearing aid aftercare sites. All hearing tests are performed at the Leeds General Infirmary or the Wharfedale/Otley Hospital.